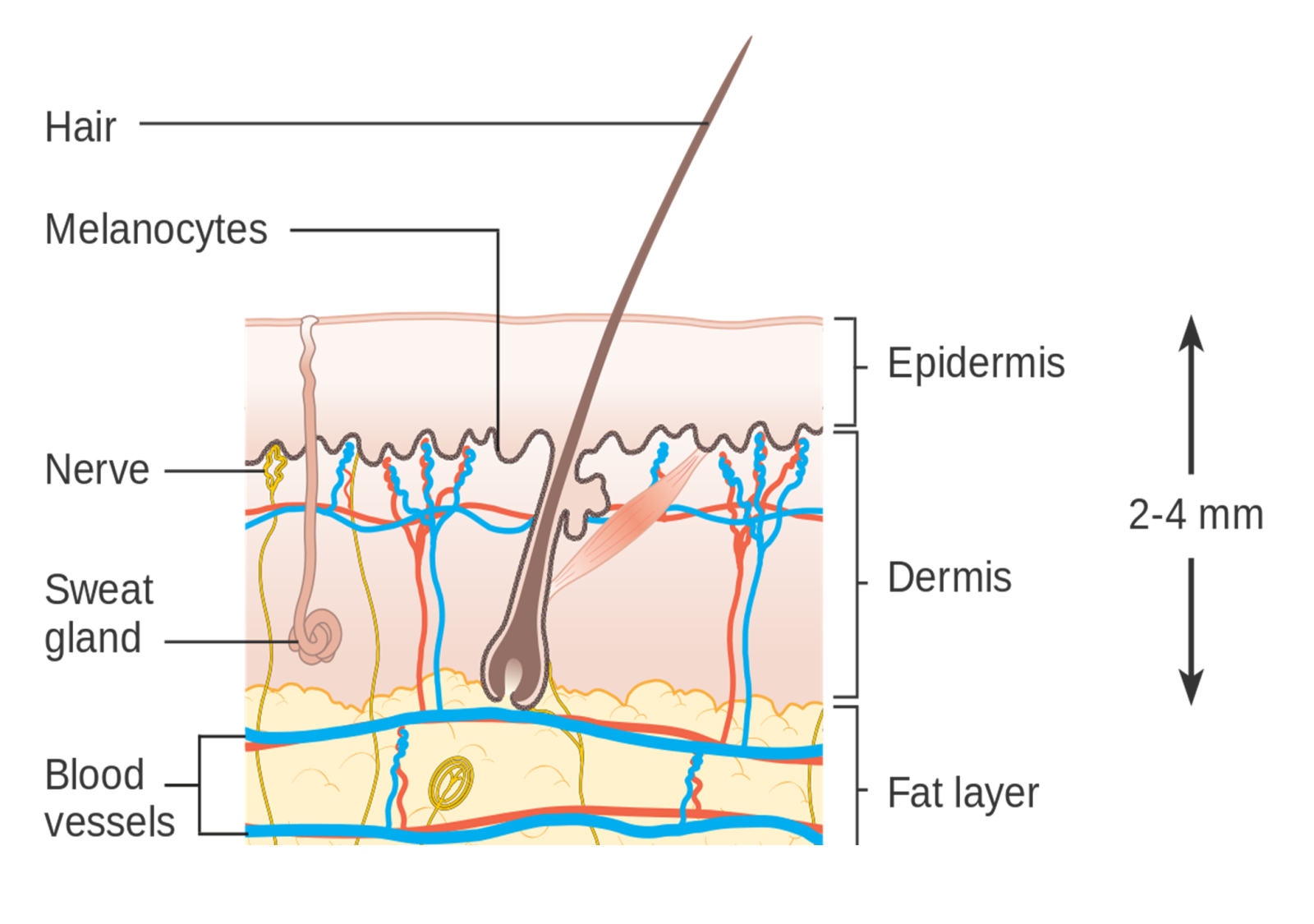
The structure of the skin
The skin is the largest organ in the body, with a surface area of 2m
2, and has multiple functions
i. The skin is composed of three layers:
- the epidermis outer layer
- the dermis middle section
- the deeper hypodermis or subcutaneous fatty layer[i]
The skin has three main functions:
- Protection
- Thermoregulation
- Sensation.[i]
The prime function of the epidermis is to:
- Act as a physical and biological barrier to the external environment
- Prevent penetration by irritants and allergens.
- Prevent the loss of water and maintains internal homeostasis.[ii]
The dermis forms the inner layer of the skin and is much thicker than the epidermis (1-5mm); its primary functions are:
- Protection
- Cushioning the deeper structures from mechanical injury
- Providing nourishment to the epidermis
- Playing an essential role in wound healing [iii].
The hypodermis consists mainly of fat with blood vessels and nerves running through it and provides
2:
- Structural support for the skin
- Insulation from the cold
- Aid in shock absorption
.png)

 Success!
Success!